GLP-1 medications like semaglutide and tirzepatide have changed the weight loss conversation. For millions of people, these drugs have produced results that diet and exercise alone never could.
But there’s a question that doesn’t get enough honest attention: what happens when you stop taking them?
The answer matters. Because if you’re considering a GLP-1 medication, or you’re already on one, understanding the weight regain data helps you plan for long-term success instead of being caught off guard six months after stopping.
The Regain Numbers: What the Research Found
The most widely cited study on GLP-1 weight regain comes from the STEP 1 trial extension, published in the journal Diabetes, Obesity and Metabolism in 2022. In that study, participants who had lost an average of about 17% of their body weight on semaglutide 2.4 mg were taken off the medication and followed for one year.
The results were sobering. Within 12 months of stopping semaglutide, participants regained roughly two-thirds of the weight they had lost. They also saw a return of the cardiometabolic improvements they’d achieved, including increases in blood pressure, blood sugar, and lipid levels.
A similar pattern showed up in the SURMOUNT-4 trial for tirzepatide, published in JAMA in 2024. Participants who switched from tirzepatide to placebo regained a significant portion of their lost weight over the following period, while those who continued the medication maintained their results.
These aren’t isolated findings. The pattern is consistent across the GLP-1 research: when you stop the medication, the weight tends to come back.
Why This Happens (It’s Not a Willpower Problem)
Weight regain after stopping GLP-1 medications isn’t about discipline or poor choices. It’s biology.
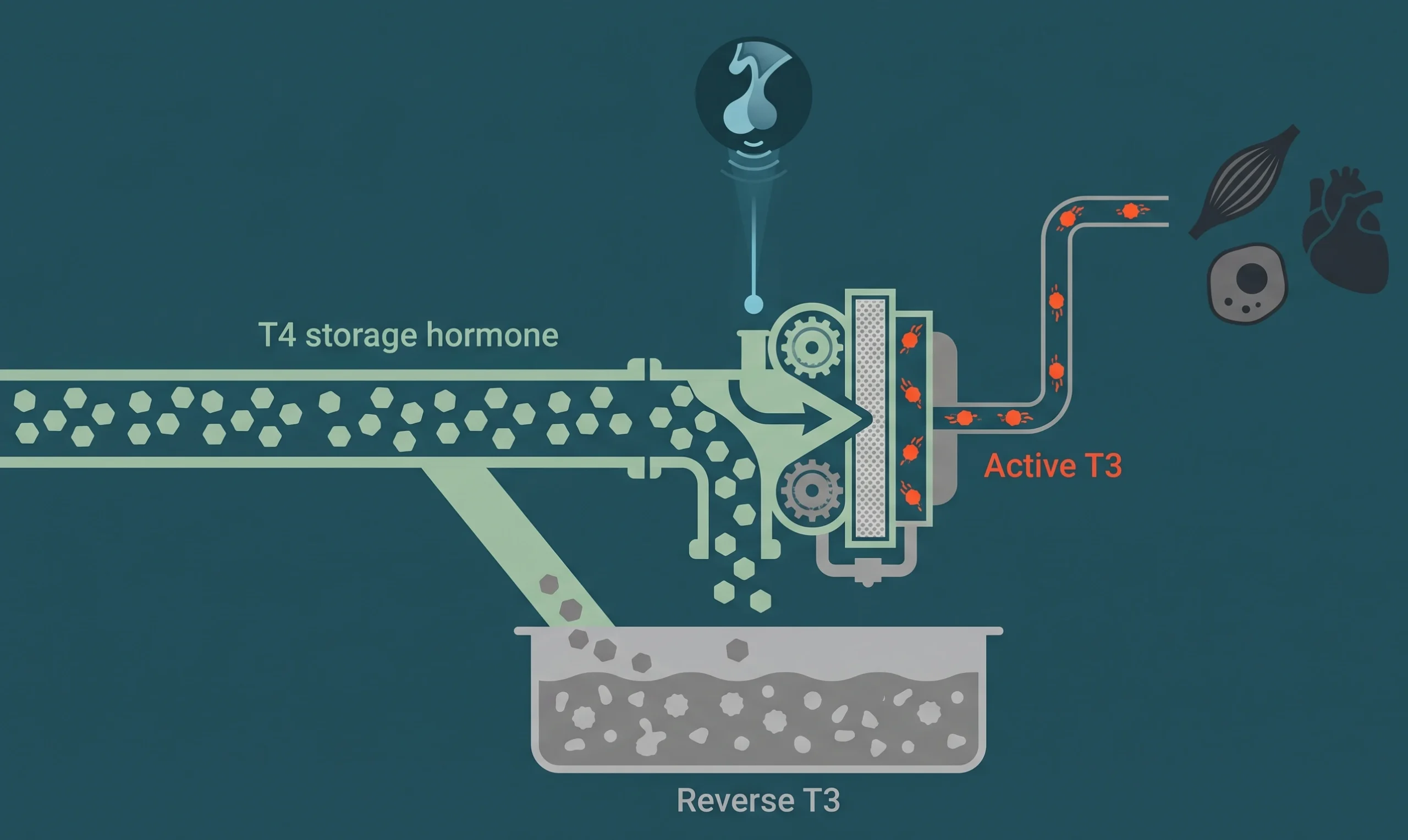
GLP-1 drugs work by mimicking a hormone your gut naturally produces. They slow gastric emptying, reduce appetite, improve insulin sensitivity, and affect hunger signaling in the brain. When you take them, your body operates in a different metabolic state. Your hunger is lower. Your satiety signals are stronger. Your blood sugar is better regulated.
When you stop, those effects disappear. Your appetite returns to its previous baseline. The hunger signals your brain was receiving get turned back up. Your metabolic set point, the weight your body defends as “normal,” reasserts itself.
This isn’t unique to GLP-1 medications. It’s the same biological challenge that makes sustained weight loss difficult regardless of the method. Your body has powerful homeostatic mechanisms that resist weight loss and promote regain. GLP-1 drugs override those mechanisms while you’re on them. Remove the override, and the mechanisms come back.
Understanding this removes the shame from the equation. Weight regain after GLP-1 discontinuation isn’t failure. It’s physiology.
What This Means for Treatment Planning
The regain data doesn’t mean GLP-1 medications are a bad choice. It means they need to be part of a broader strategy, not the entire strategy.
Think of it this way. If you had high blood pressure and a medication brought it under control, you wouldn’t expect to stop the medication and have your blood pressure stay low permanently. Obesity and metabolic dysfunction work similarly. For many people, these are chronic conditions that benefit from ongoing management.
This is why physician-supervised weight loss matters so much more than getting a prescription from an online pharmacy and figuring the rest out on your own. The medication is a tool. What happens around that tool determines whether the results last.
The Strategies That Reduce Regain Risk
While no approach eliminates regain risk entirely, the clinical evidence and the experience of physicians who manage these protocols daily point to several strategies that make a meaningful difference.
Gradual dose reduction instead of abrupt stopping. Some practitioners taper patients off GLP-1 medications rather than discontinuing them suddenly. While formal clinical trial data on tapering protocols is still limited, the rationale is sound. A gradual reduction gives the body time to adjust to lower levels of appetite suppression rather than experiencing a sudden return of full hunger signaling.
Building muscle during treatment, not just losing fat. One of the concerns with GLP-1 medications is that a portion of the weight lost is lean mass (muscle), not just fat. Muscle is metabolically active tissue. The more of it you lose, the lower your resting metabolic rate drops, and the easier it becomes to regain weight.
Resistance training during GLP-1 treatment helps preserve and build lean mass. This isn’t optional if long-term results matter. It’s a core part of the strategy. Adequate protein intake supports this as well. Most guidelines suggest aiming for higher protein targets during weight loss to protect muscle tissue.
Addressing hormonal factors that drive weight regain. This is where most GLP-1 prescribers drop the ball. Weight management doesn’t exist in a hormonal vacuum.
Low testosterone in men contributes to fat storage and muscle loss. Estrogen and progesterone shifts during perimenopause and menopause change where women store fat and how efficiently they metabolize it. Thyroid dysfunction slows metabolism. Insulin resistance makes fat storage the default mode.
If these hormonal drivers aren’t identified and addressed alongside GLP-1 treatment, they work against you the moment the medication stops. Hormone optimization isn’t a separate conversation from weight management. It’s the same conversation.
Metabolic monitoring throughout treatment. Tracking more than just the number on the scale helps identify problems before they become setbacks. Fasting insulin, hemoglobin A1c, inflammatory markers, and body composition measurements (not just weight) provide a clearer picture of metabolic health. A patient whose scale weight looks good but whose insulin resistance is worsening has a regain problem waiting to happen.
Behavior and lifestyle changes that stick. GLP-1 medications create a window of reduced appetite that makes behavior change easier. The question is whether patients use that window to build sustainable habits or simply enjoy the reduced hunger without changing anything else.
Sleep optimization, stress management, meal timing, food quality, and consistent movement patterns all contribute to long-term weight maintenance. None of these are revolutionary. But implementing them while appetite is suppressed is dramatically easier than trying to adopt them while fighting constant hunger.
The Role of Long-Term, Lower-Dose Maintenance
One emerging approach in the clinical community is the use of lower maintenance doses of GLP-1 medications after initial weight loss goals are achieved. Instead of stopping the medication entirely, patients step down to a lower dose that maintains appetite regulation without the full therapeutic dose.
This approach is gaining traction because it aligns with how we treat other chronic conditions. The clinical trials support it: in SURMOUNT-4, patients who continued tirzepatide maintained their weight loss while those who stopped regained. The practical question is finding the lowest effective dose that preserves results while minimizing cost and potential side effects.
This is a conversation to have with your physician, not a decision to make based on what you read online. The right maintenance approach depends on your starting point, your metabolic profile, your hormonal status, and how your body responds over time.
What the Online Clinics Get Wrong
The explosion of telehealth GLP-1 prescribers has made access easier. But access without context is a problem.
Many online clinics prescribe semaglutide or tirzepatide with minimal evaluation and no plan for what happens after the weight comes off. They don’t check hormone levels. They don’t measure body composition. They don’t monitor metabolic markers beyond basic labs. And they don’t have a strategy for the transition off medication.
This is how people end up in the regain cycle. They lose 30 or 40 pounds, feel great, stop the medication (sometimes because of cost), and watch the weight come back over the next year. Then they blame themselves when the real problem was a lack of planning.
A physician who treats weight loss as a metabolic and hormonal challenge, not just an appetite problem, builds a protocol that accounts for what happens at every stage, including the stage after the medication stops or is reduced.
The Honest Conversation Worth Having
If you’re on a GLP-1 medication or considering one, here are the questions worth asking your provider:
What’s the plan for when I reach my target weight? If the answer is “we’ll figure it out then,” that’s not a plan.
Are we monitoring anything beyond my weight? Body composition, hormone levels, and metabolic markers matter more than the number on the scale.
Am I doing enough to protect my muscle mass? If resistance training and protein intake aren’t part of the conversation, a significant piece is missing.
Have my hormones been evaluated? Untreated hormonal imbalances make long-term weight maintenance harder regardless of what medication you’re taking.
Is there a maintenance strategy? Whether that’s a lower dose, a different medication, or a transition protocol supported by hormonal and metabolic optimization, there should be a plan.
The Bottom Line on GLP-1 Weight Regain
GLP-1 medications work. The weight loss they produce is real and, for many people, life-changing. But the data is equally clear that stopping these medications without a plan leads to significant regain in the majority of cases.
This doesn’t mean you’ll be on medication forever. It means that sustainable results require more than a prescription. They require a strategy that addresses the hormonal, metabolic, and behavioral factors that determine whether the weight stays off.
The best outcomes happen when GLP-1 therapy is one piece of a larger plan, not the entire plan.
Build a Plan That Lasts
If you want weight loss results that hold up over time, the work starts with understanding what’s driving your weight gain in the first place. Hormones, metabolism, body composition, and lifestyle factors all play a role.
Schedule a consultation to discuss a weight management approach that goes beyond the prescription and gives you a real strategy for long-term success.