There is a clinical pattern that shows up over and over in optimization-focused practices. A woman in her early 40s walks in for hormone therapy evaluation. During the intake, she mentions she has been on an SSRI for two or three years. When she is asked why she started, the answer follows a recognizable script.
She told her primary care that she was anxious, not sleeping, irritable in a way that was new for her. The doctor ran a TSH and a basic blood panel. Everything came back normal. The doctor prescribed an SSRI, with the explanation that this was likely stress-related anxiety or mild depression. The medication helped for a while. Then it plateaued, or stopped working entirely, or worked acceptably while side effects accumulated (weight gain, sexual side effects, emotional flattening).
The woman accepted this as her new normal. Then she started bioidentical progesterone, sometimes estradiol, sometimes both. Within weeks or months, the symptoms that brought her to the SSRI in the first place changed. With her psychiatrist or primary care guiding the taper, she came off the SSRI. She did not need it anymore.
This is not a universal pattern. SSRIs are appropriate treatments for clinical depression and several anxiety disorders. They save lives, and tapering off them requires medical supervision and careful judgment. But the pattern is common enough that it deserves to be discussed openly. What follows is the mechanism behind it and what an evaluation looks like for a woman who wonders if her diagnosis missed something.
What Hormones Do to the Brain
The brain runs on a complex set of neurotransmitter and neuromodulator systems, and the major reproductive hormones interact with several of them directly.
Progesterone, through its metabolite allopregnanolone, modulates the GABA-A receptor. GABA is the brain’s primary inhibitory neurotransmitter. When GABA activity drops, the system runs hotter. Anxiety, sleep disruption, and a sense of being unable to wind down all become more likely. When progesterone is steady, the GABA system has a consistent modulator. When progesterone drops or fluctuates wildly (the early perimenopause pattern), the GABA system loses that stabilizer.
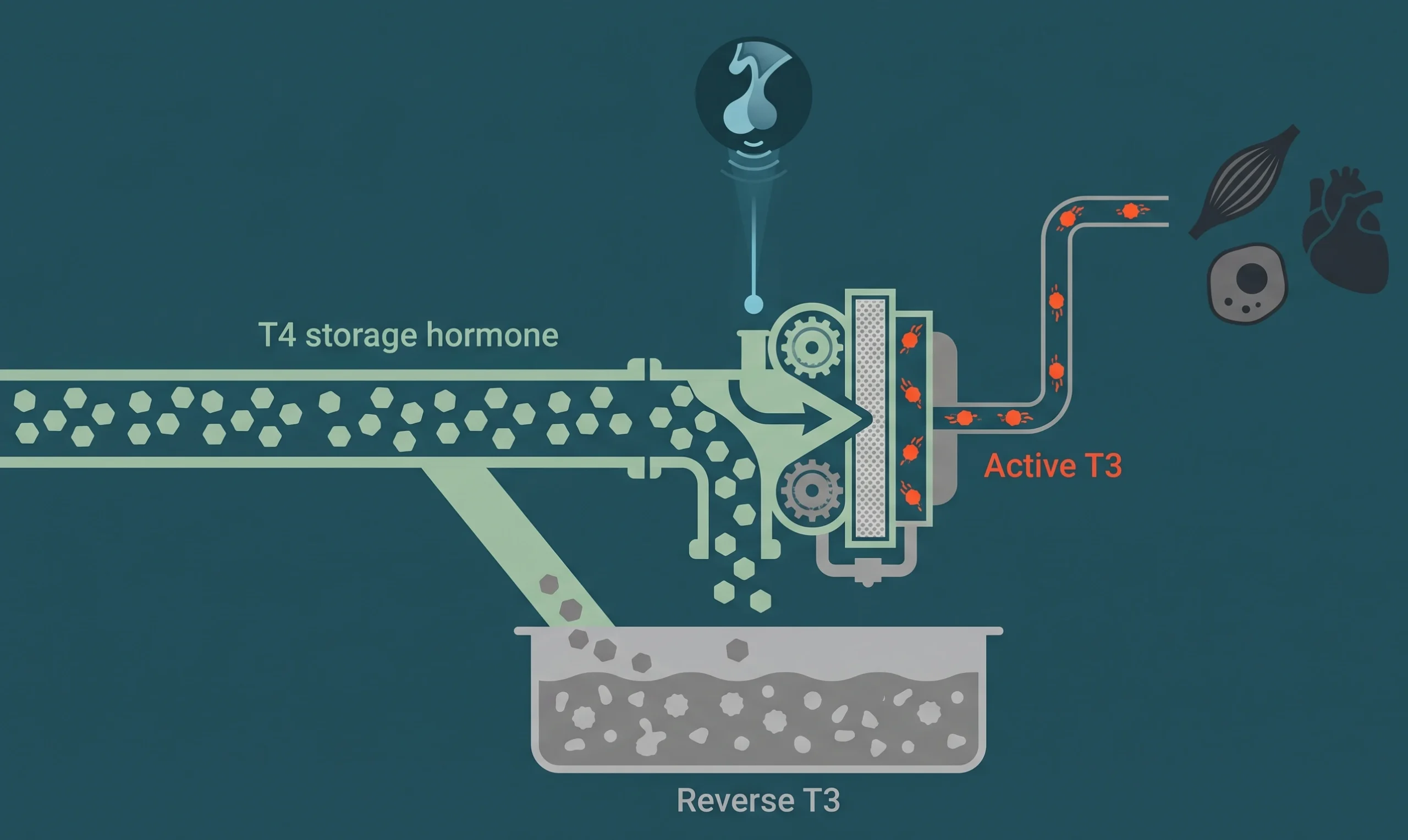
Estradiol affects multiple systems. It influences serotonin transporter density, which is one of the targets SSRIs act on. It also affects dopamine signaling and noradrenergic activity. Stable estradiol provides a kind of baseline regulation across these systems. Fluctuating estradiol, which is the hallmark of mid-perimenopause, produces variable neurotransmitter signaling that the patient experiences as mood instability, brain fog, and emotional reactivity that does not match the situation.
This is well-documented neuroendocrine biology. It is not controversial in the research literature. The disconnect is that it does not consistently make it into primary care evaluations of new-onset anxiety in midlife women.
The Perimenopause Pattern That Looks Like Depression
The hormonal changes that begin in early perimenopause produce a symptom pattern that overlaps significantly with anxiety and depression diagnostic criteria.
Sleep disruption is one of the earliest symptoms. The 3 AM wake-up that becomes a regular occurrence is often a progesterone signal, not a stress signal.
New-onset anxiety, especially in a woman who has not previously been particularly anxious, is another early sign. The anxiety often feels novel. It does not have an obvious trigger. It shows up despite a life situation that has not meaningfully changed.
Irritability that surprises the patient. She finds herself snapping at her family or coworkers in ways that feel out of character.
Loss of interest in things that previously felt rewarding. This is often subtle and gets attributed to being too busy or burned out.
Reduced concentration and word-finding difficulty. This shows up clinically as brain fog and gets attributed to stress.
Changes in libido and energy that the patient often does not bring up unless asked.
Looking at this list, every item is also on standard depression and anxiety screening tools. A patient presenting with these symptoms will reliably score in the range that suggests medication. If the conversation does not specifically include “where are you in your menstrual cycle history” and “have we tested your hormone status,” the hormonal driver gets missed by design.
The perimenopause symptom post goes deeper into the missed-diagnosis patterns. The pattern this post focuses on is specifically the SSRI prescription that followed.
Why SSRIs Were Studied for Menopause Symptoms
It is worth saying clearly that SSRIs have real evidence in menopause care. Paroxetine has an FDA approval for moderate-to-severe vasomotor symptoms (hot flashes) under the brand name Brisdelle. Venlafaxine, an SNRI, has been studied for the same indication.
The evidence base for SSRIs reducing hot flash frequency is real. For women who cannot take hormone therapy due to specific contraindications (active breast cancer being the clearest one), these medications are legitimate options.
What the evidence does not support is the assumption that an SSRI is a first-line response to perimenopause-pattern anxiety, sleep disruption, and mood symptoms in a woman who is a candidate for hormone therapy. The SSRI is treating a downstream symptom. The hormonal fluctuation that is driving the symptom remains unaddressed.
What Bioidentical Progesterone Does in This Population
For a woman whose primary symptoms are sleep disruption, anxiety, and irritability that started in her early 40s, oral micronized progesterone at bedtime is often the most useful single intervention.
The mechanism connects back to the GABA modulation discussed earlier. Allopregnanolone is the active metabolite produced when oral progesterone is processed by the liver. It modulates the GABA-A receptor in ways that promote sleep onset, sleep maintenance, and a calming effect that patients describe as feeling more settled in their own body.
This is one of the more reliably reported clinical effects in perimenopause hormone therapy. It is not subtle. Women who respond often describe the change as feeling like they got their old self back.
The choice between progesterone and a synthetic progestin matters here. The two molecules do not produce the same effect, which we covered in the progesterone versus progestin breakdown. If you have been on a progestin (oral contraceptive, Provera, the Mirena IUD progestin) and felt off, that is a different experience than what bioidentical progesterone tends to produce.
Adding Estradiol in the Right Cases
For women in mid-perimenopause whose estrogen has begun to swing more dramatically, adding transdermal estradiol can address the symptoms that progesterone alone does not. Brain fog, mood instability that progresses through the day, vasomotor symptoms, and the cognitive issues that begin to surface all respond to estrogen stabilization in many cases.
The decision to add estradiol depends on the patient’s specific presentation, her risk profile, and where she is on the perimenopause timeline. The decision is not made on symptoms alone. A workup that includes the actual hormone levels and the patient’s history is the input.
The Important Caveats
Three caveats are essential and have to be said clearly.
First, this pattern does not apply to every woman on an SSRI. Some women are on antidepressants for clinical depression that predates perimenopause, for treatment-resistant conditions, or for diagnoses unrelated to reproductive hormones. Hormone therapy is not going to replace an SSRI for major depressive disorder. The pattern this post describes is specifically the woman who started an SSRI in her late 30s or 40s for what was characterized as new-onset anxiety and whose hormones were never evaluated.
Second, tapering an SSRI requires medical supervision. SSRI discontinuation syndrome is real, and the taper has to be paced. The clinician who evaluates whether the patient is ready to taper is usually the prescriber. The hormone therapy clinician’s role is to address the hormonal driver. The two providers should communicate.
Third, the goal is not to get a patient off medications she actually needs. The goal is to confirm the diagnosis was right in the first place. For some women, the SSRI was the right call and remains the right call. For others, the hormonal driver was missed, and once it is addressed, the SSRI may become unnecessary. The evaluation is what determines which group a patient is in.
What an Evaluation Looks Like
For a woman currently on an SSRI who suspects hormones may be part of her picture, an evaluation includes:
A detailed history of when the symptoms started, what they felt like, and what was happening hormonally at that time (menstrual cycle changes, premenstrual symptom intensification, sleep changes correlated with cycle phases).
A hormone panel that goes beyond TSH. Estradiol, progesterone (timed appropriately if still cycling), SHBG, total and free testosterone, DHEA-S, and the full thyroid panel.
A review of the current SSRI experience: how it has helped, what residual symptoms remain, what side effects have accumulated.
A conversation with the patient about goals, risk tolerance, and what a hormone trial would look like.
If hormone therapy is appropriate, a plan that introduces it carefully and coordinates with the SSRI prescriber on a possible taper if and when symptoms support it.
The perimenopause treatment program handles exactly this kind of case routinely. The intake is structured to ask the questions a typical 15-minute primary care visit does not have time for.
The Honest Position
This post is not an argument against antidepressants. It is an argument that women whose symptoms started in their late 30s or 40s deserve to have their hormonal status evaluated before, or alongside, an antidepressant prescription. That step has been missing from a lot of primary care interactions for decades.
If you are on an SSRI that you suspect was prescribed for what was actually a hormonal pattern, the evaluation to know for sure is straightforward. Book a consultation and we will start with the labs and the history that should have been part of the original conversation.