There is a frustrating routine that plays out in primary care offices every day. A patient comes in tired, cold, gaining weight, losing hair, struggling to focus. The doctor orders TSH. It comes back at 2.4. The patient is told their thyroid is normal and the symptoms must be something else. Stress. Aging. Sleep. Maybe a referral to mental health.
The problem with this exchange is that TSH was never a thyroid hormone. It is a brain signal. And a normal brain signal does not prove the rest of the system is working.
This is the gap where a lot of patients get lost for years. The labs say normal. The body says otherwise. Both can be true.
What TSH Actually Measures
TSH stands for thyroid stimulating hormone. It is produced by the pituitary gland in response to feedback from circulating thyroid hormone levels. When the pituitary senses that thyroid hormone is low, it releases more TSH to push the thyroid harder. When thyroid hormone is high, TSH drops.
So TSH is not measuring your thyroid. It is measuring whether your brain thinks your thyroid is producing enough. That is a useful screen for primary disease (the thyroid itself failing) and for severe overproduction. It is much less useful for catching subtle conversion problems downstream.
This is why TSH became the default. It is cheap, the assay is reliable, and it catches the cases primary care needs to catch first. The American Thyroid Association supports TSH-first screening for most adults, and from a population-health standpoint, that position is reasonable. The trade-off is that anyone whose problem is not at the pituitary-to-thyroid step gets missed.
The T4 to T3 Conversion Problem
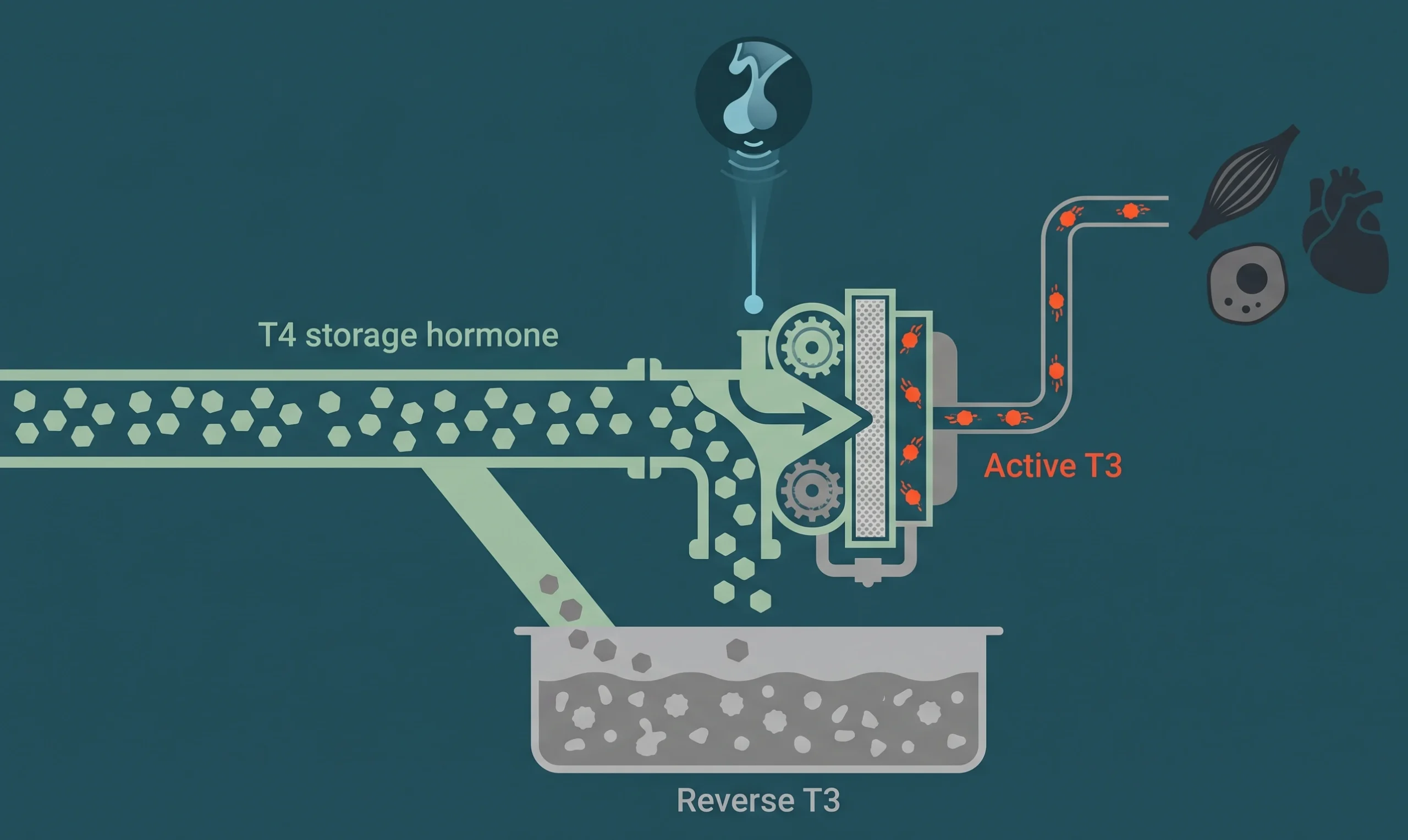
Your thyroid produces mostly T4, which is best understood as a storage form. T4 has to convert into T3 (the active form) before any cell in your body can use it. That conversion happens in the liver, the gut, the kidneys, and at the cellular level, regulated by enzymes called deiodinases.
A lot of things can interfere with that conversion:
- High cortisol from chronic stress
- Inflammation (often driven by gut issues, autoimmunity, or visceral fat)
- Low ferritin (iron stores)
- Low selenium and zinc
- Restrictive dieting and chronic calorie deficit
- Heavy alcohol use
- Some medications, including beta blockers and amiodarone
When conversion is impaired, you can have a beautiful TSH and a normal free T4 while your tissues are starving for active hormone. The blood test that catches this is free T3.
Free T3 is the unbound, biologically available form of the active hormone. If TSH says the brain is happy and free T4 says the storage tank is full but free T3 is sitting at the bottom of the reference range, you have a conversion problem, not a production problem. The treatment for those two scenarios is completely different. So is the prognosis if you ignore them.
The Reverse T3 Escape Valve
There is a second reason free T3 can be low while everything else looks normal. Under stress, illness, or chronic inflammation, the body shunts T4 into reverse T3 instead of T3. Reverse T3 is structurally similar to active T3 but does not activate the receptor. Worse, it competes with T3 at the receptor site. So elevated reverse T3 acts as a brake on whatever T3 you do have.
This pattern is common in:
- High-cortisol states (chronic stress, demanding careers, poor sleep)
- Recent illness or surgery
- Aggressive caloric restriction
- Athletic overtraining
- Chronic inflammation from any source
You will not see this on a standard panel because reverse T3 is not part of one. You have to specifically request it. We covered this and the rest of the missed markers in the hormone labs most doctors skip.
In-Range Versus Ideal: Why Functional Medicine Pushes Higher
Lab reference ranges are statistical. They are built from a large pool of people and represent two standard deviations around the average. The problem is that the pool includes plenty of people with subclinical thyroid issues. So “normal” by lab standards includes a lot of subtly dysfunctional thyroid status.
Functional and optimization-focused medicine takes a different position. The argument is that healthy thyroid function corresponds to free T3 in the upper third of the reference range, not the lower third. There are patients who feel hypothyroid at a free T3 of 2.6 (when the lab range is 2.0 to 4.4) and feel fine at 3.6.
This is not universally accepted in mainstream endocrinology, and the evidence base is mixed. But the clinical experience of treating patients in the optimization range is hard to ignore. The patient who has been tired for five years, has been told their labs are fine repeatedly, and starts feeling like themselves again when free T3 moves into the upper range is making a fairly clear empirical case.
Symptom Patterns That Suggest Functional Hypothyroidism
When TSH is normal but the patient is functionally hypothyroid, the symptom picture tends to follow a recognizable pattern:
- Cold hands and feet, especially in the morning
- Hair thinning at the outer third of the eyebrows (a classic thyroid sign)
- Slow morning recovery, taking hours to feel awake even after a full night’s sleep
- Persistent constipation that does not respond well to fiber and water
- Dry skin and brittle nails
- Weight gain that does not respond to caloric reduction the way it used to
- A morning resting heart rate that runs lower than expected
- A basal body temperature that consistently runs below 97.8 degrees Fahrenheit
Any one of these in isolation is not specific. The cluster is harder to explain by anything other than thyroid status.
The Cortisol Connection
There is one more variable that ties most of this together. Chronic high cortisol is one of the strongest drivers of poor T4-to-T3 conversion. The mechanism is well-described: cortisol upregulates the deiodinase that converts T4 to reverse T3 instead of T3. So a patient with HPA axis dysregulation will often present with normal TSH, low-normal free T3, and elevated reverse T3.
Treating the thyroid in this scenario without addressing the cortisol pattern usually fails. The thyroid medication adds T4 to a system that is busy converting T4 into reverse T3. The patient might feel marginally better for a few weeks and then plateau.
This is a common reason patients on T4-only therapy feel like the medication “stopped working.” It did not stop working. The conversion step has gotten worse. For the executive avatar who is running on caffeine and four hours of poor sleep, this is the rule, not the exception.
What a Full Thyroid Panel Looks Like
If you want a real picture of thyroid function, the panel needs to go beyond TSH. At Towsen Clinic, the full thyroid workup pulls:
- TSH
- Free T4
- Free T3
- Reverse T3
- TPO antibodies (catches Hashimoto’s even when TSH is still acceptable)
- Thyroglobulin antibodies (catches a smaller subset of autoimmune thyroid disease)
The interpretation considers the relationship between markers, not just whether each one is in range. Free T3 in the bottom 20% of the reference range with elevated reverse T3 and a normal TSH is a clear functional pattern, even though every individual number would be called “normal” on a primary care report.
The treatment plan depends on the pattern. Sometimes it is T3 supplementation. Sometimes it is addressing cortisol and inflammation so the body’s own conversion can recover. Sometimes it is iron, selenium, or another nutrient input. Often it is a combination, sequenced over several months. There is no single thyroid protocol that works for every patient, and any clinic that offers one should be approached with skepticism. We see this overlap with cortisol dysregulation often enough that it shows up in nearly every workup, which is part of why our hormone optimization program starts with a panel broad enough to catch the full pattern.
If you have been told repeatedly that your thyroid is “fine” while you continue to feel anything but, the missing piece is usually the conversion step. Book a thyroid-focused consultation and we will run the labs that show what TSH alone cannot.