There is a generation of women, now in their 50s and 60s, who avoided hormone therapy because of a press conference held in July 2002. The Women’s Health Initiative (WHI) released preliminary findings from its combined estrogen-plus-progestin arm, the study was halted early for safety, and the headlines that followed told women that hormone therapy caused breast cancer and heart disease.
The headlines were not entirely wrong, but they were profoundly incomplete. Two decades of follow-up data have rewritten most of the original conclusions. The medical literature has shifted. The major menopause societies have updated their positions. Most primary care offices have not caught up.
If you have been hesitant about hormone therapy because of what you heard 20 years ago, the picture you have is almost certainly outdated. Here is what the data actually showed, what got distorted, and what the current evidence supports.
What the WHI Actually Studied
The WHI was launched in the 1990s as one of the largest women’s health studies ever undertaken. It enrolled more than 16,000 postmenopausal women in the combined hormone arm, which was the part of the study that made the 2002 headlines. The trial compared women taking a daily combination of conjugated equine estrogen (the brand name Premarin, derived from horse urine) plus medroxyprogesterone acetate (the brand name Provera, a synthetic progestin) against women taking a placebo.
Two details about the study population are essential and were almost never mentioned in the press coverage. The average age of women enrolled was 63, and many were more than a decade past menopause. The trial was not studying women in their 40s and early 50s beginning hormone therapy near the time of their final period. It was studying older women starting hormone therapy long after menopause.
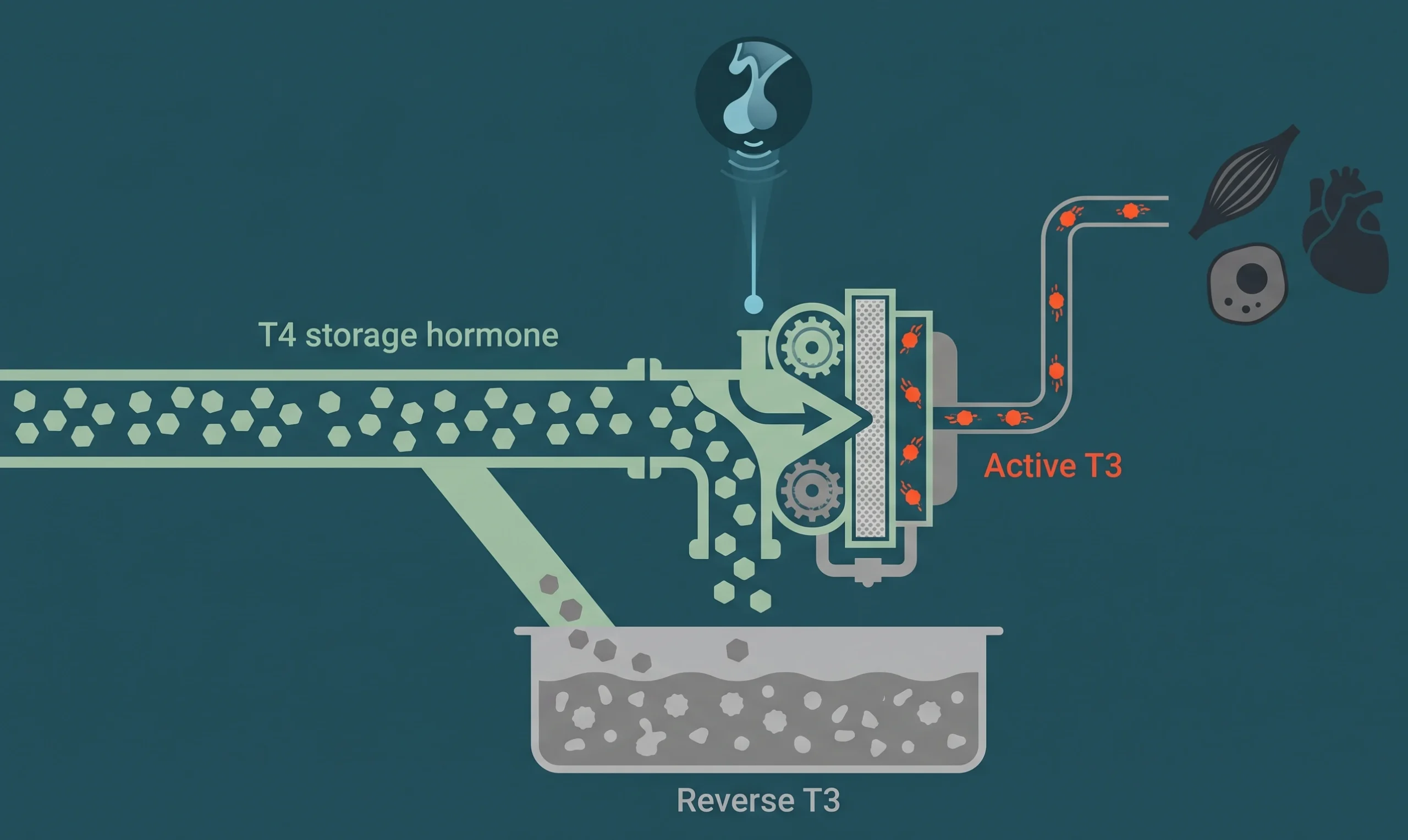
The other detail that mattered: the specific drugs used. Conjugated equine estrogen and medroxyprogesterone acetate are not the same molecules the ovaries produce. They are synthetic or animal-derived compounds with different pharmacology than the bioidentical hormones used in most modern protocols. We covered this distinction in detail in the post on bioidentical versus synthetic hormones.
The combined arm was halted in 2002 after the data safety monitoring board determined that the risks (a small increase in breast cancer, cardiovascular events, and stroke) outweighed the benefits at the interim analysis. The press release went out the same day. The nuance did not survive the news cycle.
The Absolute Versus Relative Risk Problem
The 2002 reporting hinged on relative risk numbers that sounded alarming and rarely came with the absolute risk context that would have calmed most readers.
A relative risk increase tells you how much more likely an event is in the treatment group compared to the control group. An absolute risk increase tells you how many more people out of every 100 or 1,000 actually experience the event. When the underlying event is rare, large relative risk numbers can correspond to tiny absolute risk numbers.
The original WHI press release reported that combined hormone therapy was associated with an increased relative risk of breast cancer. The absolute risk worked out to fewer than 1 additional breast cancer case per 1,000 women per year. That is a real number and it deserves attention, but it is not the kind of risk that should have ended hormone therapy as a category. It was, in the original publication, smaller than the breast cancer risk associated with obesity or with two daily glasses of wine.
The headlines did not include the second number. The conversation moved on without it. Two generations of women lost access to a treatment that, in the right population and with the right protocol, has a very different risk profile.
The Estrogen-Only Arm That Got Buried
The WHI had a second arm that enrolled women who had previously had a hysterectomy and could safely take estrogen alone (without a progestogen, since the uterus was no longer present and there was no endometrial cancer risk to manage). This arm took conjugated equine estrogen alone.
The findings from the estrogen-only arm were dramatically different from the combined arm. There was no significant increase in breast cancer. In some follow-up analyses, there was actually a reduction. The cardiovascular results were also more favorable, especially in women who initiated therapy closer to menopause.
This arm of the study received a fraction of the press coverage. The combined-therapy headlines had already shaped the public conversation. The estrogen-only data, which suggested that the progestin (not the estrogen) was likely responsible for much of the increased breast cancer signal, never reached most patients. Even today, many women still believe that estrogen itself causes breast cancer. The WHI data does not actually support that conclusion when estrogen is studied on its own.
The Timing Hypothesis
The largest reframing of the WHI data has come from what is called the timing hypothesis. The argument is that the age at which hormone therapy is initiated dramatically affects the risk-benefit ratio.
For women who begin hormone therapy within 10 years of menopause or before age 60, the cardiovascular outcomes look quite different from women who begin therapy more than a decade past menopause. The biological argument is that estrogen has protective effects on vascular tissue when started before significant atherosclerotic disease has developed. Started after that disease is established, estrogen can interact with unstable plaque in ways that increase event risk.
This explains a large portion of the WHI cardiovascular signal. The average woman in the WHI combined arm was 63 at enrollment, with many having been postmenopausal for 10 to 20 years. Re-analyses that stratified the data by age at initiation found that younger initiators had a different cardiovascular profile than older initiators. The pooled headline number combined both groups and obscured the difference.
For a woman in her early 50s today considering hormone therapy near the time of her final menstrual period, the WHI cardiovascular concern is much less applicable than the headlines suggested. She is in the lower-risk window. This is one of the central reasons we keep emphasizing the timeline in our perimenopause timeline post. Where you are on the timeline matters.
What the Major Societies Now Say
The North American Menopause Society (NAMS), the Endocrine Society, and the American College of Obstetricians and Gynecologists have all updated their positions over the past 15 years to reflect the follow-up data. The current consensus, broadly stated:
For symptomatic women within 10 years of menopause or under age 60, the benefits of hormone therapy often outweigh the risks for treatment of vasomotor symptoms, genitourinary symptoms, and the prevention of bone loss. The risk-benefit calculation shifts unfavorably the further from menopause therapy is initiated.
The choice of formulation matters. Transdermal estradiol (a patch or gel) has a different risk profile than oral conjugated equine estrogen, particularly for clotting risk. Micronized progesterone has a different risk profile than medroxyprogesterone acetate, particularly for breast tissue effects. Modern protocols at optimization-focused clinics generally use the formulations with the better-evidence safety profiles.
This is a meaningful change from the blanket “avoid hormone therapy” message that defined the 2000s. Most patients have not been told it has changed.
What This Means for a Woman Considering Hormone Therapy Today
If you are in your 40s or early 50s, perimenopausal or recently menopausal, and you have been told repeatedly that hormone therapy is too risky to even discuss, the data does not support that blanket position. The actual conversation requires:
A real risk-benefit assessment based on your personal and family history. A woman with a strong personal history of estrogen-receptor-positive breast cancer is in a different conversation than a woman with no such history. Both deserve nuanced evaluation rather than reflexive avoidance.
A clear understanding of which formulation is being prescribed. Bioidentical estradiol delivered transdermally with oral micronized progesterone is not the same as oral conjugated equine estrogen with medroxyprogesterone acetate. The data on these two protocols looks substantially different. We go into the bioidentical specifics on the bioidentical hormone therapy page.
A frank conversation about timing. Starting hormone therapy within a few years of your final menstrual period is a different decision than starting 15 years after. The biology is different. The risk-benefit numbers are different.
An ongoing monitoring plan. Hormone therapy is not “set it and forget it.” Periodic reassessment of symptoms, lab markers, and risk factors is part of responsible care.
The Honest Position
There is no version of medicine where hormone therapy is risk-free for every woman. There is also no version of the WHI data, even the original 2002 publication read in full, that justifies the categorical avoidance that became the cultural default.
If you have been told for 20 years that hormone therapy will give you breast cancer or a heart attack, the source of that message is almost certainly a misreading of a single study from 2002. The current evidence is more nuanced, and for many women in the right window, the calculation favors treatment.
If you are considering hormone therapy and want a genuine evaluation rather than reflexive avoidance or reflexive prescription, book a consultation and we will work through the actual data that applies to your situation.