You’re not lazy. You’re not burned out because you lack willpower. And you’re not imagining it.
But if you’re a high earner running on fumes, that fatigue is costing you more than you think. Not just in how you feel, but in actual dollars, missed opportunities, strained relationships, and years of compounding losses that most people never stop to calculate.
Fatigue is one of the most expensive health problems nobody tracks. There’s no line item for it on your tax return. No invoice from your body at the end of the quarter. But when you start adding up the real costs, the number is staggering.
The Productivity Tax You’re Already Paying
Here’s something most professionals don’t realize. Showing up to work tired costs more than not showing up at all.
Researchers call this “presenteeism,” being physically present but mentally and physically underperforming. A RAND Corporation study found that fatigue-related productivity loss costs the U.S. economy hundreds of billions of dollars annually. And at the individual level, the impact is just as real.
Think about your own workday when you’re exhausted. Decisions take longer. Emails sit unanswered. Creative thinking shrinks to a minimum. You default to the easiest option instead of the best one. Meetings blur together. You leave work feeling like you accomplished half of what you planned.
Now multiply that across weeks, months, and years.
If you earn $250,000 annually and you’re operating at 70% capacity due to chronic fatigue, the gap between what you’re producing and what you could produce is enormous. That’s not a precise formula. It’s a thought exercise. But it illustrates something important: fatigue doesn’t just make you tired. It makes you less effective at the thing that generates your income.
The Career Opportunities You’re Not Seeing
The productivity tax is the cost you can measure. The opportunity cost is the one you can’t.
When you’re exhausted, you stop volunteering for the stretch assignments. You pass on the conference that could lead to your next client. You skip the networking dinner because you don’t have the energy to be “on” for another three hours. You let the younger colleague take the lead on the new initiative because you just don’t have it in you today.
None of these feel like major decisions in the moment. But over time, they add up to a pattern of pulling back. And in competitive fields where visibility, initiative, and energy signal leadership potential, pulling back has real consequences.
Promotions, partnerships, board seats, new business relationships: these go to the people who show up with energy and presence. Not the people who are technically competent but visibly running on empty.
For professionals earning $175,000 to $400,000 or more, even a single missed promotion or lost client relationship can represent tens of thousands of dollars in forgone income. And that’s before you factor in the compounding effect on future earnings.
The Healthcare Costs That Pile Up Quietly
Chronic fatigue doesn’t just affect your work. It drives a cascade of healthcare spending that most people don’t connect to the root cause.
When you’re exhausted, you’re more likely to get sick. Your immune system runs on sleep and hormonal balance, and when those are disrupted, you’re more vulnerable to infections, longer recovery times, and chronic inflammation.
Fatigue also drives compensatory behaviors that have their own costs. More caffeine. More sugar. More alcohol to wind down at night. Less exercise because you’re too tired to make it to the gym. Poor food choices because cooking takes energy you don’t have.
These patterns lead to weight gain, metabolic dysfunction, sleep disorders, and mood issues, each of which generates its own round of doctor visits, prescriptions, and specialist referrals. You end up treating symptoms of symptoms, never addressing the actual cause.
Many high earners spend thousands of dollars per year on supplements, sleep gadgets, biohacking tools, and wellness subscriptions trying to fix fatigue on their own. Some of these help at the margins. But none of them replace finding out why you’re exhausted in the first place.
The Relationship Costs Nobody Talks About
This is the one that hits hardest, and it’s almost never discussed in financial terms.
When you’re chronically tired, your patience shrinks. Small annoyances become arguments. You’re less present with your kids. Date nights feel like obligations instead of opportunities. Intimacy declines, not because you don’t care, but because you have nothing left to give by the end of the day.
Over time, this erodes the relationships that matter most. And while you can’t put a dollar figure on a marriage or a child’s trust, you can recognize that the cost of fatigue extends far beyond your bank account.
For the professionals who are already worried about being “present enough” for their families, this is often the pain point that finally pushes them to seek help. Not the work performance. Not the weight gain. The moment they realize they’re physically there but emotionally absent.
Why Fatigue Isn’t “Just Stress”
The standard response to chronic fatigue in high performers is predictable. “You’re working too hard.” “You need to manage your stress better.” “Try meditation.”
These suggestions aren’t wrong, exactly. Stress management matters. But they miss the bigger picture.
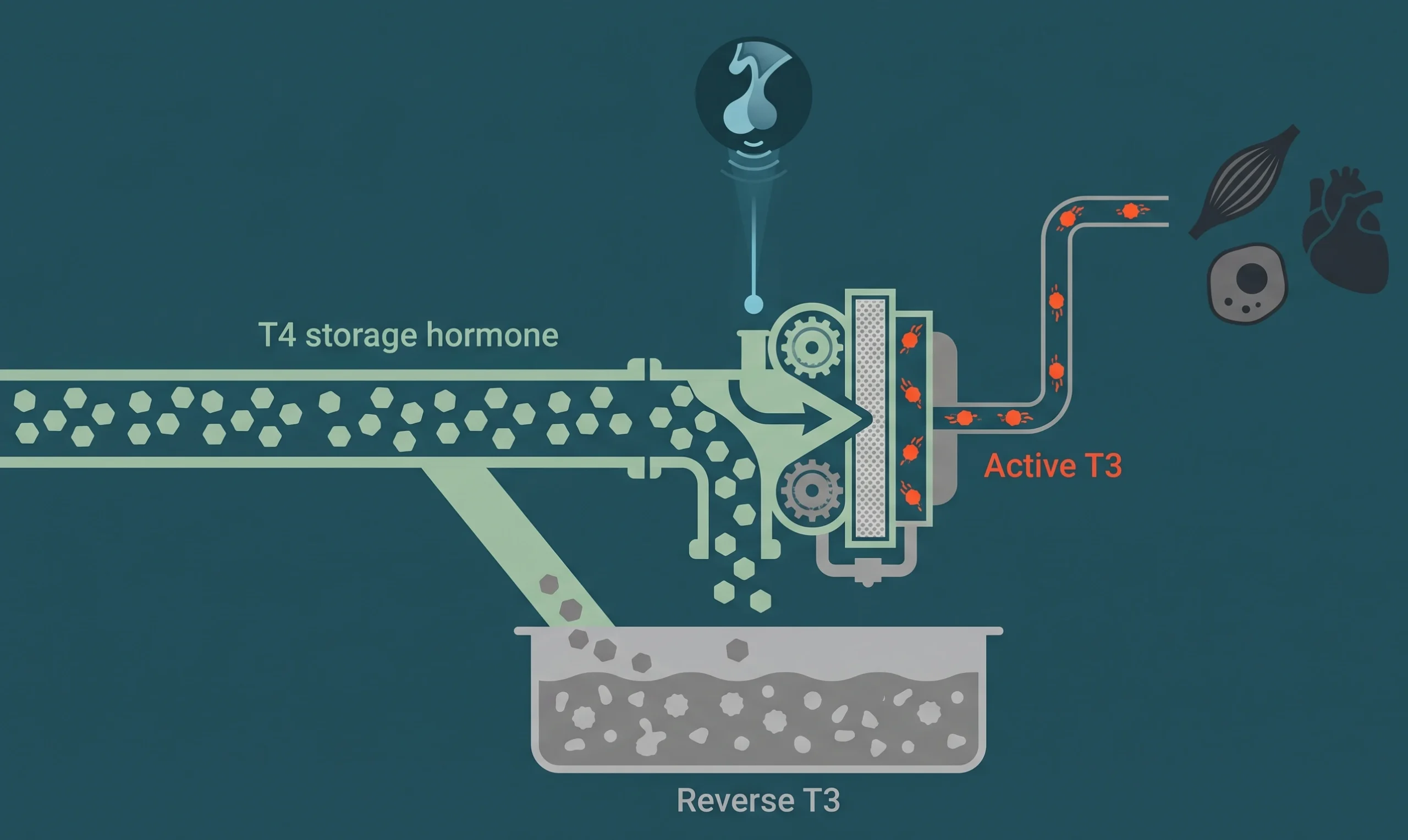
For many men and women over 40, chronic fatigue has a physiological driver that no amount of meditation will fix. Declining testosterone, shifting estrogen and progesterone levels, underperforming thyroid function, insulin resistance, and nutrient deficiencies can all produce relentless fatigue, even in people who are doing everything “right” from a lifestyle perspective.
This is the frustrating part. You eat well. You exercise when you can. You try to sleep enough. And you’re still dragging. That’s not a willpower problem. That’s a signal that something in your body needs attention.
The challenge is that most primary care doctors don’t test for these underlying causes in any meaningful depth. A standard metabolic panel and a TSH check barely scratch the surface. And when those results come back “normal,” you’re told to reduce stress and come back in a year.
Meanwhile, the fatigue continues. And the costs keep compounding.
The Compounding Effect Over a Decade
Consider a 45-year-old professional earning $300,000 per year who’s been dealing with moderate fatigue for three years. They’ve already experienced reduced productivity, passed on at least a few career opportunities, spent extra money on healthcare and symptom management, and absorbed strain in their closest relationships.
Now imagine that fatigue continues unchecked for another five to ten years. The productivity gap widens. The career trajectory flattens or declines. Health problems multiply as metabolic and hormonal issues worsen. Relationship damage becomes harder to reverse.
Compare that to the same person who identifies the root cause early, addresses it, and gets back to performing at full capacity. The difference in lifetime earnings, career trajectory, health outcomes, and relationship quality is enormous.
This is why framing fatigue as a minor inconvenience is so costly. It’s not a bad week you’ll bounce back from. For many people, it’s a slow, compounding drain that affects every area of life.
Treating Fatigue as the Investment Problem It Actually Is
High earners are trained to think in terms of return on investment. They analyze deals, evaluate risk, and allocate capital based on expected outcomes.
But when it comes to their own health, many of them tolerate years of subpar performance without ever investigating the cause. They’ll spend hours analyzing a $50,000 business decision and zero hours investigating why they can barely function after lunch.
Health optimization reframes this equation. The cost of a thorough evaluation and, if needed, a treatment protocol is a fraction of what chronic fatigue costs you in lost productivity, missed opportunities, and declining health.
Think of it this way. If a financial advisor told you there was a portfolio issue silently draining 20 to 30% of your returns, you’d want to know about it immediately. Chronic fatigue is doing the same thing to your most valuable asset: your ability to perform, earn, and show up fully in your life.
What Finding the Root Cause Looks Like
Solving chronic fatigue starts with asking better questions and running better tests.
A proper evaluation includes a full hormone panel, thyroid markers beyond basic TSH, metabolic indicators, inflammatory markers, and a detailed review of your symptoms, lifestyle, and health history.
This isn’t a 15-minute appointment. It’s a thorough process designed to find what’s actually driving your fatigue, not just rule out the most obvious possibilities.
Once the cause is identified, treatment can be targeted and effective. For some people, that means hormone optimization. For others, it means addressing metabolic dysfunction, nutrient deficiencies, or sleep-disrupting hormone imbalances. Often, it’s a combination.
The point is that fatigue has a cause. And causes can be treated. “Getting older” is not a diagnosis. It’s a dismissal.
Stop Accepting the Cost
You wouldn’t tolerate a 30% efficiency loss in your business for years without investigating. You shouldn’t tolerate it in your body either.
Chronic fatigue isn’t something you manage around. It’s something you solve. And solving it pays dividends in every area of your life: sharper work, better relationships, improved health, and more energy for the things that matter.
If you’re ready to find out what’s actually driving your exhaustion, schedule a consultation to get the answers you’ve been missing.