Hormone therapy has changed dramatically in the past decade. The fear-driven era following the 2002 Women’s Health Initiative is giving way to a more nuanced, evidence-based approach that focuses on optimization rather than just replacement.
But what does the current research actually show about outcomes? What are patients experiencing? And what separates a good result from a great one?
This post pulls together findings from published clinical studies, professional society guidelines, and emerging research to give you a clear picture of where hormone optimization therapy stands right now and what realistic outcomes look like.
The Shift from Replacement to Optimization
For decades, hormone therapy had one goal: bring deficient levels back into the “normal” range. If your testosterone was below 264 ng/dL or your estradiol had bottomed out, you got treatment. If your levels fell somewhere inside the reference range, you were considered fine, regardless of how you felt.
That model is fading. A growing number of physicians now recognize that the reference range is a statistical tool, not a clinical target. The question is shifting from “Are you deficient?” to “Are you at the level where you function best?”
This shift matters because the outcomes data tells a consistent story: patients who are treated to personalized targets report better results than those who are simply brought to the lower end of the normal range.
The Endocrine Society, the American Urological Association, and the North American Menopause Society have all updated their guidelines in recent years to reflect a more individualized approach. The direction of the field is clear, even if adoption across primary care is still catching up.
Testosterone Therapy Outcomes: What the Studies Show
Testosterone therapy for men has some of the strongest outcome data in the hormone optimization space. Here’s what the major studies have found.
Energy and fatigue. The Testosterone Trials (TTrials), a coordinated set of seven clinical trials funded by the National Institutes of Health, found that testosterone therapy improved self-reported energy and vitality in men over 65 with low testosterone. Participants reported meaningful improvements in physical activity and reduced fatigue over the 12-month study period.
Body composition. Research consistently shows that testosterone therapy reduces fat mass and increases lean body mass. A meta-analysis published in Clinical Endocrinology reviewed multiple randomized controlled trials and confirmed that testosterone treatment produces significant reductions in body fat percentage and increases in lean muscle, particularly in men with documented low levels.
Mood and cognitive function. The TTrials also measured mood outcomes and found that testosterone therapy improved depressive symptoms in men with low testosterone and mild depression. Separate research published in the Journal of Clinical Endocrinology and Metabolism has shown improvements in spatial memory and verbal fluency in hypogonadal men treated with testosterone.
Sexual function. This is one of the most consistently demonstrated benefits. The TTrials reported improvements in sexual desire, erectile function, and sexual activity. Multiple meta-analyses confirm these findings across different populations and age groups.
Cardiovascular safety. The TRAVERSE trial, published in the New England Journal of Medicine in 2023, was a landmark study specifically designed to assess cardiovascular safety. It followed over 5,000 men with hypogonadism and preexisting or high risk for cardiovascular disease. The study found that testosterone therapy did not increase the risk of major cardiovascular events compared to placebo. This was a significant finding that addressed years of uncertainty.
Hormone Therapy Outcomes for Women: What the Evidence Supports
Women’s hormone therapy research has accelerated significantly since the WHI. The picture is far more positive than the 2002 headlines suggested.
Vasomotor symptoms. Hot flashes and night sweats remain the most common reason women seek hormone therapy, and the evidence for effectiveness is robust. The Cochrane Collaboration’s systematic review confirmed that hormone therapy reduces the frequency and severity of hot flashes by approximately 75%. Both bioidentical and synthetic formulations show effectiveness, though the safety profiles differ.
Sleep quality. Sleep disruption during perimenopause and menopause is extremely common and often underappreciated. Studies published in Menopause: The Journal of the North American Menopause Society show that hormone therapy, particularly when it includes progesterone, improves sleep quality, reduces nighttime awakenings, and increases total sleep time.
Bone health. Estrogen therapy remains one of the most effective interventions for preventing postmenopausal bone loss. The WHI itself confirmed that hormone therapy significantly reduced fracture risk, a finding that even critics of the study acknowledge.
Cognitive function. The research here is more complex. Data suggests that hormone therapy started close to menopause onset (the “critical window hypothesis”) may have cognitive protective effects, while therapy started many years after menopause may not offer the same benefits. The KEEPS (Kronos Early Estrogen Prevention Study) and ELITE trials support the idea that timing matters significantly.
Mood and well-being. Multiple studies confirm that hormone therapy improves mood, reduces anxiety, and enhances overall quality of life in perimenopausal and postmenopausal women. This is consistent with what clinicians observe: women who were struggling with perimenopause symptoms often report feeling like themselves again within weeks to months of starting therapy.
What Separates Good Outcomes from Great Ones
Not all hormone therapy produces the same results. The clinical evidence, combined with what experienced practitioners observe, points to several factors that consistently predict better outcomes.
Starting earlier tends to produce better results. The critical window hypothesis applies broadly. Men and women who address hormonal decline when symptoms first appear, rather than waiting years, tend to respond faster and more completely. Waiting until age 60 to address issues that started at 45 means the body has been compensating and declining for 15 years.
Personalized dosing outperforms standard protocols. Studies comparing fixed-dose therapy to individually adjusted protocols consistently show that personalized approaches produce better symptom relief with fewer side effects. This is because hormone needs vary widely between individuals based on genetics, body composition, stress levels, and metabolic health.
Monitoring makes a measurable difference. Patients who receive regular lab monitoring and dosage adjustments report better sustained outcomes than those on “set it and forget it” protocols. Hormones fluctuate, and protocols that adapt to those changes keep patients in their ideal range over time.
Addressing multiple systems together produces compounding benefits. Testosterone doesn’t work in isolation. Neither does estrogen. Research increasingly supports what optimization physicians have long observed: addressing hormones, metabolic health, sleep, and lifestyle factors together produces outcomes that are greater than what any single intervention achieves alone.
The provider’s expertise matters enormously. A 2020 survey published in Maturitas found that many primary care physicians feel undertrained in hormone therapy management. Patients treated by physicians with specialized training in hormone optimization report higher satisfaction and better clinical outcomes. This is not a critique of primary care. It’s a recognition that hormone optimization is a specialty skill set.
The Numbers That Matter Most
If you’re considering hormone therapy, the benchmarks worth paying attention to aren’t just hormone levels. The metrics that correlate most strongly with patients feeling and functioning their best include:
Free testosterone (not just total) for men. As we’ve discussed in previous posts, total testosterone can look “normal” while free testosterone is too low to support how you want to feel.
Estradiol levels for women (and men). Too low causes symptoms. Too high causes different symptoms. The target depends on the individual and the delivery method.
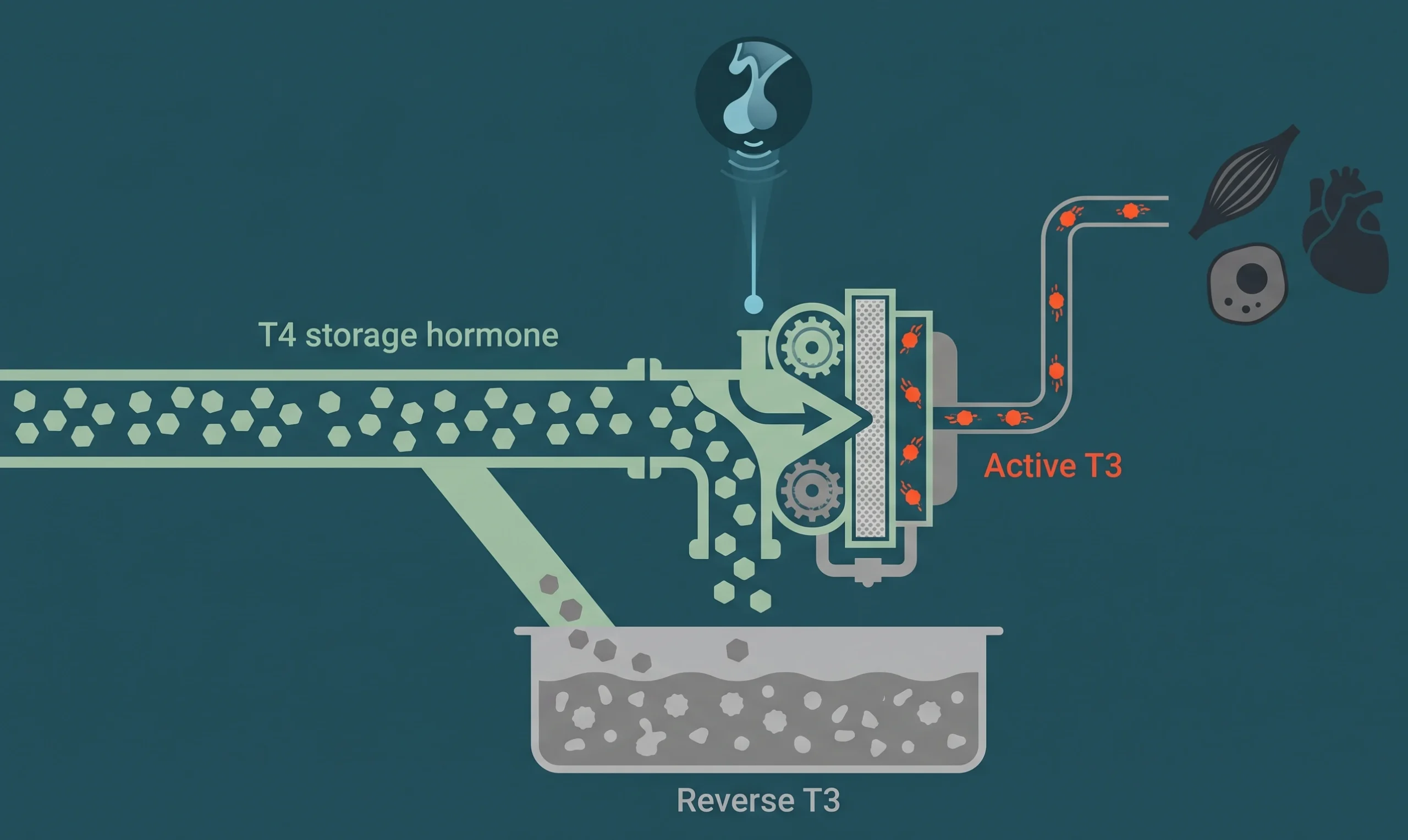
Thyroid function beyond TSH. Free T3, free T4, and thyroid antibodies tell a much fuller story than TSH alone. Suboptimal thyroid function mimics and amplifies hormone deficiency symptoms.
Inflammatory markers. Chronic inflammation interferes with hormone receptor sensitivity. High-sensitivity C-reactive protein (hs-CRP) and other markers can reveal why therapy isn’t producing expected results.
Metabolic markers. Fasting insulin, hemoglobin A1c, and lipid panels help identify metabolic resistance that can blunt the benefits of hormone therapy.
Sleep quality metrics. Poor sleep undermines every other intervention. Tracking sleep architecture, not just hours in bed, provides actionable data.
Where the Field Is Heading
Several trends are shaping the future of hormone optimization.
Better testing technology. Advances in lab testing, including dried blood spot testing and more sensitive assays, are making it easier to track hormone levels with precision and convenience.
Integration with peptide therapy. Peptide protocols are increasingly being combined with hormone therapy to address recovery, sleep, body composition, and cognitive function. The evidence base for peptides like BPC-157, CJC-1295, and others continues to grow.
Greater emphasis on the gut-hormone connection. Emerging research on the gut microbiome’s influence on hormone metabolism is opening new avenues for optimizing therapy outcomes.
Wider acceptance among mainstream medicine. As studies like TRAVERSE and the updated menopause society guidelines continue to validate the safety and efficacy of hormone therapy, more providers are offering it and more patients are seeking it.
AI and data-driven personalization. Some clinics are beginning to use pattern recognition across patient data to refine protocols faster. While still early, this trend could accelerate the shift from population-based dosing to truly individualized care.
What This Means for You
The state of hormone therapy in 2026 is more promising than it’s ever been. The research is stronger. The safety data is more reassuring. The protocols are more sophisticated. And the outcomes, when therapy is managed properly, are consistently positive.
If you’ve been hesitant because of outdated fears, misinformation, or a bad experience with a provider who wasn’t specialized in this area, the landscape has changed. The evidence supports what patients have been reporting for years: when hormones are optimized properly, people feel better, perform better, and age better.
The question isn’t whether hormone optimization works. The research has answered that. The question is whether you’re getting the right evaluation, the right protocol, and the right monitoring to get the results the evidence says are possible.
Find Out Where You Stand
You don’t need to guess about your hormone levels or wonder whether therapy might help. A thorough evaluation gives you real numbers and a clear picture of what’s happening in your body.
Schedule a consultation to review your labs, discuss your symptoms, and learn what an evidence-based optimization protocol could do for you.